DIAGNÓSTICO Y SEGUIMIENTO DE LA HIPERTENSIÓN ARTERIAL PULMONAR [2024]
DESCARGAR
VERSIÓN EXTENSA
DESCARGAR
ANEXOS
DESCARGAR
VERSIÓN CORTA
DESCARGAR RECOMENDACIONES Y FLUJOGRAMAS
vacio
vacio
Ámbito
•El ámbito asistencial incluye los establecimientos de salud del tercer nivel de atención de EsSalud.
Población y alcance
- Pacientes con sospecha sintomática y diagnóstico de hipertensión arterial pulmonar.
Autores
Grupo elaborador
Expertos clínicos:
- Oscar Nellson Aguirre Zurita
Médico cardiólogo, Instituto Nacional Cardiovascular “Carlos Alberto Peschiera Carrillo”, EsSalud, Lima, Perú - Marcos Rodrigo Padilla Reyes
Médico cardiólogo, Hospital Nacional Edgardo Rebagliati Martins, EsSalud, Lima, Perú - Victoria Celeste Armas Rodríguez
Médico cardiólogo, Hospital Nacional Arzobispo Loayza, Ministerio de Salud, Lima, Perú - Miriam Milagros Valdez Ramos
Médico cardiólogo, Hospital María Auxiliadora, Ministerio de Salud, Lima, Perú - Nassip Carlojusto Llerena Navarro
Médico cardiólogo, Hospital Nacional Carlos Alberto Seguín Escobedo, EsSalud, Arequipa, Perú - Jorge Luis Jara Valderrama
Médico cardiólogo, Hospital Víctor Lazarte Echegaray, EsSalud, La Libertad, Perú - Noelia Cacho Maldonado
Médico cardiólogo, Hospital Departamental de Huancavelica, Ministerio de Salud, Huancavelica, Perú - Tatiana Gisell Coca Caycho
Médico intensivista, Hospital Nacional Almanzor Aguinaga Asenjo, EsSalud, Lambayeque, Perú - Alexander Montesinos Cárdenas
Médico cardiólogo, Hospital Nacional «Adolfo Guevara Velasco», EsSalud, Cusco, Perú - Genaro Gustavo Grajeda Valdez
Médico cardiólogo, Hospital Nacional «Adolfo Guevara Velasco», EsSalud, Cusco, Perú - Kenyi Rolando Salas Sotelo
Médico cardiólogo, Hospital Nacional «Adolfo Guevara Velasco», EsSalud, Cusco, Perú - Ciro Alberto Barrantes Alarcón
Médico cardiólogo, Hospital Nacional Guillermo Almenara Irigoyen, EsSalud, Lima, Perú
Metodólogos:
- Wendy Carolina Nieto Gutiérrez
Metodóloga, IETSI, EsSalud, Lima, Perú - Daniel Aarón Fernández Guzmán
Metodólogo, IETSI, EsSalud, Lima, Perú - Lelis Gabriela Coronel Chucos
Metodóloga, IETSI, EsSalud, Lima, Perú
Metodología
Resumen de la metodología:
- Conformación del GEG: La Dirección de Guías de Práctica Clínica, Farmacovigilancia y Tecnovigilancia, del Instituto de Evaluación de Tecnologías en Salud e Investigación (IETSI) del Seguro Social del Perú (EsSalud), conformó un grupo elaborador de la guía (GEG), que incluyó médicos especialistas y metodólogos.
- Planteamiento de preguntas clínicas: En concordancia con los objetivos y alcances de esta GPC, se formularon las preguntas clínicas.
- Búsqueda de la evidencia para cada pregunta: Para cada pregunta clínica, se realizaron búsquedas de revisiones sistemáticas (publicadas como artículos científicos o guías de práctica clínica). De no encontrar revisiones de calidad, se buscaron estudios primarios, cuyo riesgo de sesgo fue evaluado usando herramientas estandarizadas.
- Evaluación de la certeza de la evidencia: Para graduar la certeza de la evidencia, se siguió la metodología Grading of Recommendations Assessment, Development, and Evaluation (GRADE), y se usaron tablas de Summary of Findings (SoF).
- Formulación de las recomendaciones: El GEG revisó la evidencia recolectada para cada una de las preguntas clínicas en reuniones periódicas, en las que formuló las recomendaciones usando la metodología GRADE, otorgándole una fuerza a cada una. Para ello, se tuvo en consideración los beneficios y daños de las opciones, valores y preferencias de los pacientes, aceptabilidad, factibilidad, equidad y uso de recursos. Estos criterios fueron presentados y discutidos, tomando una decisión por consenso o mayoría simple. Asimismo, el GEG emitió puntos de buenas prácticas clínicas (BPC) sin una evaluación formal de la evidencia, y mayormente en base a su experiencia clínica.
- Revisión externa: La presente GPC fue revisada en reuniones con profesionales representantes de otras instituciones, tomadores de decisiones, y expertos externos.
Flujogramas que resumen el contenido de la GPC

vacio
vacio
1. Velocidad de regurgitación tricuspídea
Descargar PDF con el desarrollo de la pregunta.
Recomendación 1:
Se recomienda el uso de la velocidad de regurgitación tricuspídea (TRVmax) de ≥2.9 m/s más ≥1 signo indirecto como alternativa para la detección de hipertensión pulmonar (HTP).
(Recomendación condicional a favor, certeza baja de la evidencia)
BPC 1:
El GEG considera que esta estrategia maximiza la detección de casos y reduce falsos negativos, siendo una alternativa más aceptable.
2. Nueva definición hemodinámica
Descargar PDF con el desarrollo de la pregunta.
Recomendación 1:
En pacientes con sospecha de hipertensión pulmonar (HTP), se sugiere adoptar la nueva definición hemodinámica con un umbral de PAPm >20 mmHg.
(Recomendación condicional a favor, certeza baja de la evidencia)
BPC 1:
Se considera que este umbral permite detecciones más tempranas y mejora la supervivencia de los pacientes.
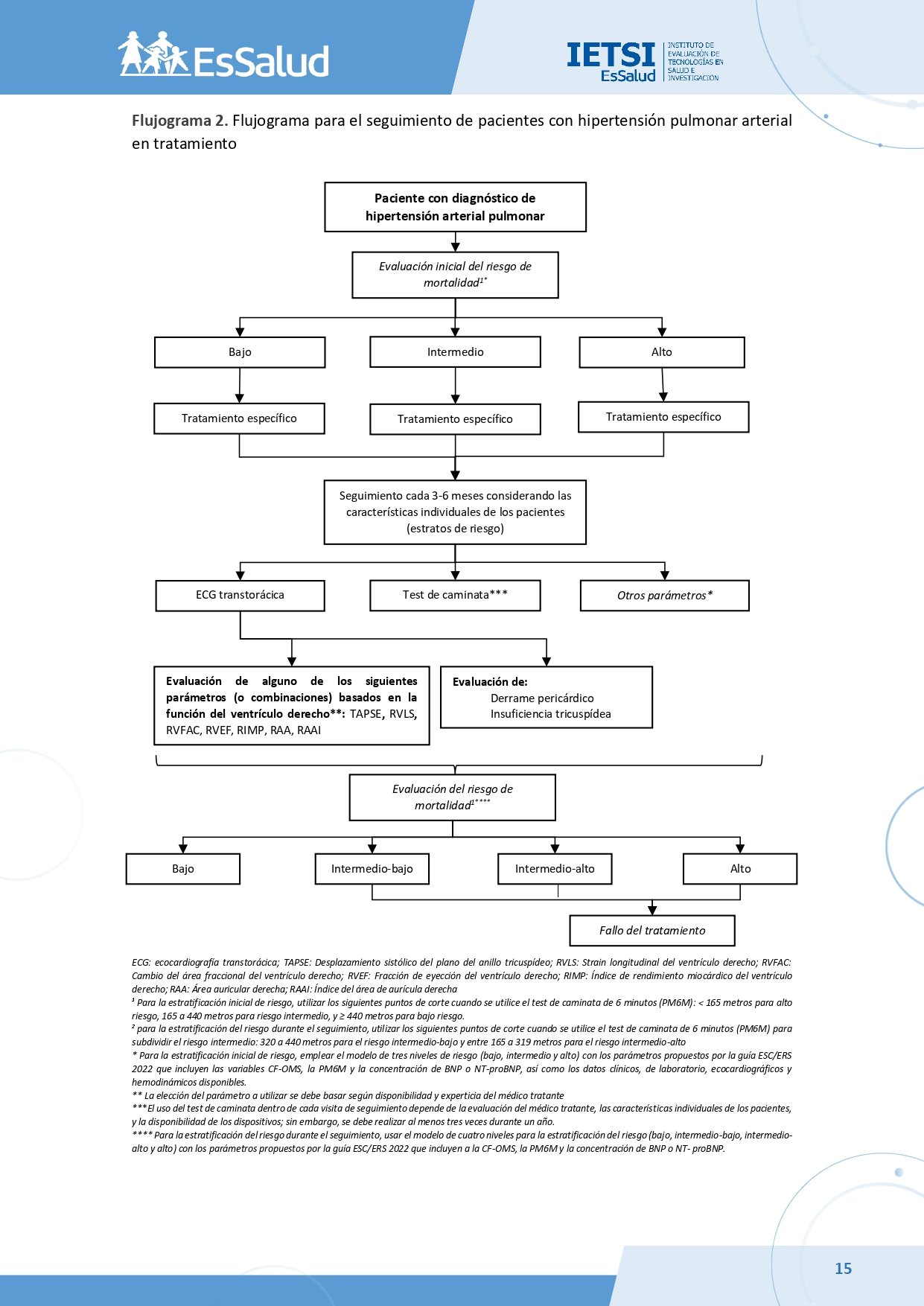
3. Estratificación de riesgo de muerte
Descargar PDF con el desarrollo de la pregunta.
Recomendación 1:
Para la estratificación del riesgo en pacientes con HTP, se sugiere usar la escala de tres niveles de la guía ESC/ERS 2022.
(Recomendación condicional a favor, certeza baja de la evidencia)
BPC 1:
El GEG también sugiere el modelo de cuatro niveles para discriminar mejor a pacientes de riesgo intermedio-alto.
4. Parámetro ecocardiográfico en respuesta a tratamiento
Descargar PDF con el desarrollo de la pregunta.
Recomendación 1:
Se recomienda el uso de la ecocardiografía para el seguimiento de pacientes con HTP.
(Recomendación fuerte a favor, certeza baja de la evidencia)
BPC 1:
Se sugiere priorizar parámetros ecocardiográficos como RVLS y RVFAC, que tienen beneficios significativos para el pronóstico.
BPC 2:
Se desaconseja el uso de RVSP debido a sus beneficios triviales y justificación limitada.
(Recomendación fuerte en contra, certeza muy baja de la evidencia)
5. Prueba de caminata de 6 minutos
Descargar PDF con el desarrollo de la pregunta.
Recomendación 1:
Se recomienda utilizar los puntos de corte <165 m, 165-440 m y >440 m en la PC6M para la estratificación del riesgo en pacientes con HTP.
(Recomendación condicional a favor, certeza baja de la evidencia)
BPC 1:
El GEG sugiere subdividir el riesgo intermedio en intermedio-bajo (320-440 m) e intermedio-alto (165-319 m) según la guía ESC/ERS 2022.
Referencias bibliográficas
1. Maron BA, Galiè N. Diagnosis, Treatment, and Clinical Management of Pulmonary Arterial Hypertension in the Contemporary Era: A Review. JAMA Cardiol. 2016;1(9):1056-65.
2. Humbert M, Kovacs G, Hoeper MM, Badagliacca R, Berger RMF, Brida M, et al. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. European Respiratory Journal. 2022:2200879.
3. Simonneau G, Gatzoulis MA, Adatia I, Celermajer D, Denton C, Ghofrani A, et al. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol. 2013;62(25 Suppl):D34-41.
4. Brouwers MC, Kho ME, Browman GP, Burgers JS, Cluzeau F, Feder G, et al. AGREE II: advancing guideline development, reporting and evaluation in health care. Canadian Medical Association Journal. 2010;182(18):E839-E42.
5. Ministerio de Salud. Documento técnico: Metodología para la de documento técnico elaboración guías de practica clínica. Lima, Perú: MINSA; 2015.
6. Shea BJ, Reeves BC, Wells G, Thuku M, Hamel C, Moran J, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. Bmj. 2017;358:j4008.
7. Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. Bmj. 2011;343:d5928.
8. Wells G, Shea B, O’connell D, Peterson J, Welch V, Losos M, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa (ON): Ottawa Hospital Research Institute; 2009. Available in March. 2016.
9. Whiting PF, Rutjes AW, Westwood ME, Mallett S, Deeks JJ, Reitsma JB, et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Annals of internal medicine. 2011;155(8):529-36.
10. Andrews JC, Schünemann HJ, Oxman AD, Pottie K, Meerpohl JJ, Coello PA, et al. GRADE guidelines: 15. Going from evidence to recommendation—determinants of a recommendation’s direction and strength. Journal of clinical epidemiology. 2013;66(7):726-35.
11. Alonso-Coello P, Schünemann HJ, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, et al. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 1: Introduction. bmj. 2016;353:i2016.
12. Alonso-Coello P, Oxman AD, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, et al. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 2: Clinical practice guidelines. bmj. 2016;353:i2089.
13. Andrews J, Guyatt G, Oxman AD, Alderson P, Dahm P, Falck-Ytter Y, et al. GRADE guidelines: 14. Going from evidence to recommendations: the significance and presentation of recommendations. Journal of clinical epidemiology. 2013;66(7):719-25.
14. Mocumbi A, Humbert M, Saxena A, Jing Z-C, Sliwa K, Thienemann F, et al. Pulmonary hypertension. Nature Reviews Disease Primers. 2024;10(1):1.
15. Rosenkranz S, Howard LS, Gomberg-Maitland M, Hoeper MM. Systemic Consequences of Pulmonary Hypertension and Right-Sided Heart Failure. Circulation. 2020;141(8):678-93.
16. Schikowski EM, Swabe G, Chan SY, Magnani JW. Association between income and likelihood of right heart catheterization in individuals with pulmonary hypertension: A US claims database analysis. Pulm Circ. 2022;12(3):e12132.
17. Dong T-X, Zhu Q, Wang S-T, Wang Y-H, Li G-Y, Kong F-X, et al. Diagnostic and prognostic value of echocardiography in pulmonary hypertension: an umbrella review of systematic reviews and meta-analyses. BMC Pulmonary Medicine. 2023;23(1):253.
18. Ni J-R, Yan P-J, Liu S-D, Hu Y, Yang K-H, Song B, et al. Diagnostic accuracy of transthoracic echocardiography for pulmonary hypertension: a systematic review and meta-analysis. BMJ Open. 2019;9(12):e033084.
19. Ullah W, Minalyan A, Saleem S, Nadeem N, Abdullah HM, Abdalla A, et al. Comparative accuracy of non-invasive imaging versus right heart catheterization for the diagnosis of pulmonary hypertension: A systematic review and meta-analysis. IJC Heart & Vasculature. 2020;29:100568.
20. Tsujimoto Y, Kumasawa J, Shimizu S, Nakano Y, Kataoka Y, Tsujimoto H, et al. Doppler trans-thoracic echocardiography for detection of pulmonary hypertension in adults. Cochrane Database Syst Rev. 2022;5(5):Cd012809.
21. Balakrishnan B, Owens B, Hayes R, Wen S. A Systematic Review of Echocardiographic Parameters for the Screening of Pulmonary Hypertension: What Are the Odds? Cureus. 2022;14(12):e32185.
22. Correale M, Rotondo C, Bevere EML, Tricarico L, Rella V, Villani D, et al. Combined peripheral and central ultrasound for the diagnosis of PAH-SSc patients. Echocardiography. 2024;41(6):e15853.
23. Mandoli GE, Landra F, Chiantini B, Sciaccaluga C, Pastore MC, Focardi M, et al. Tricuspid Regurgitation Velocity and Mean Pressure Gradient for the Prediction of Pulmonary Hypertension According to the New Hemodynamic Definition. Diagnostics. 2023;13(16):2619.
24. van de Veerdonk MC, Vonk-Noordegraaf A, Vachiery J-L. Unbowed, unbent, unbroken: predicting pulmonary hypertension using echocardiography. European Respiratory Journal. 2022;60(2):2200481.
25. Björkman A, Lund LH, Faxén UL, Lindquist P, Venkateshvaran A. Accuracy and diagnostic performance of doppler echocardiography to estimate mean pulmonary artery pressure in heart failure. Echocardiography. 2021;38(9):1624-31.
26. Montané BE, Fiore AM, Reznicek EC, Jain V, Jellis C, Rokadia H, et al. Optimal Tricuspid Regurgitation Velocity to Screen for Pulmonary Hypertension in Tertiary Referral Centers. CHEST. 2021;160(6):2209-19.
27. Gall H, Yogeswaran A, Fuge J, Sommer N, Grimminger F, Seeger W, et al. Validity of echocardiographic tricuspid regurgitation gradient to screen for new definition of pulmonary hypertension. eClinicalMedicine. 2021;34.
28. Sumimoto K, Tanaka H, Mukai J, Yamashita K, Tanaka Y, Shono A, et al. Optimal Cut-Off of Tricuspid Regurgitation Velocity According to the New Definition of Pulmonary Hypertension - Its Use in Predicting Pulmonary Hypertension. Circ Rep. 2020;2(10):625-9.
29. Sitbon O, Humbert M, Nunes H, Parent F, Garcia G, Hervé P, et al. Long-term intravenous epoprostenol infusion in primary pulmonary hypertension: prognostic factors and survival. J Am Coll Cardiol. 2002;40(4):780-8.
30. AVOUAC J, AIRÒ P, MEUNE C, BERETTA L, DIEUDE P, CARAMASCHI P, et al. Prevalence of Pulmonary Hypertension in Systemic Sclerosis in European Caucasians and Metaanalysis of 5 Studies. The Journal of Rheumatology. 2010;37(11):2290-8.
31. Kubota K, Miyanaga S, Akao M, Mitsuyoshi K, Iwatani N, Higo K, et al. Association of delayed diagnosis of pulmonary arterial hypertension with its prognosis. J Cardiol. 2024;83(6):365-70.
32. Hoeper MM, Lee SH, Voswinckel R, Palazzini M, Jais X, Marinelli A, et al. Complications of right heart catheterization procedures in patients with pulmonary hypertension in experienced centers. J Am Coll Cardiol. 2006;48(12):2546-52.
33. EsSalud. Catalogo de tarifas de prestaciones de salud a terceros no asegurados. Lima, Perú: EsSalud.
34. Ivarsson B, Johansson A, Kjellström B. The Odyssey from Symptom to Diagnosis of Pulmonary Hypertension from the Patients and Spouses Perspective. J Prim Care Community Health. 2021;12:21501327211029241.
35. Morrisroe K, Stevens W, Sahhar J, Rabusa C, Nikpour M, Proudman S. Epidemiology and disease characteristics of systemic sclerosis-related pulmonary arterial hypertension: results from a real-life screening programme. Arthritis Res Ther. 2017;19(1):42.
36. Krowka MJ, Fallon MB, Kawut SM, Fuhrmann V, Heimbach JK, Ramsay MA, et al. International Liver Transplant Society Practice Guidelines: Diagnosis and Management of Hepatopulmonary Syndrome and Portopulmonary Hypertension. Transplantation. 2016;100(7):1440-52.
37. Rich S, Haworth SG, Hassoun PM, Yacoub MH. Pulmonary hypertension: the unaddressed global health burden. The Lancet Respiratory Medicine. 2018;6(8):577-9.
38. Xue L, Yang Y, Sun B, Liu B, Zeng Q, Xiong C. Mildly Elevated Pulmonary Arterial Pressure Is Associated With a High Risk of Progression to Pulmonary Hypertension and Increased Mortality: A Systematic Review and Meta-Analysis. J Am Heart Assoc. 2021;10(7):e018374.
39. Lin P, Jiang F, Li X, Zhao Y, Shi Y, Liang Z. International trends in pulmonary hypertension mortality between 2001 and 2019: Retrospective analysis of the WHO mortality database. Heliyon. 2024;10(4):e26139.
40. Hernández F, Larrosa J, Nacazume J, Aguirre O, Larrea N, Franco-Watanabe S, et al. Costo de la hipertensión arterial pulmonar en el Perú. Revista de la Facultad de Medicina Humana. 2021;21:580-7.
41. Galiè N, Humbert M, Vachiery J-L, Gibbs S, Lang I, Torbicki A, et al. Guía ESC/ERS 2015 sobre diagnóstico y tratamiento de la hipertensión pulmonar. Revista Española de Cardiología. 2016;69(2):177.e1-.e62.
42. Kylhammar D, Kjellström B, Hjalmarsson C, Jansson K, Nisell M, Söderberg S, et al. A comprehensive risk stratification at early follow-up determines prognosis in pulmonary arterial hypertension. European Heart Journal. 2017;39(47):4175-81.
43. Boucly A, Weatherald J, Savale L, Jaïs X, Cottin V, Prevot G, et al. Risk assessment, prognosis and guideline implementation in pulmonary arterial hypertension. Eur Respir J. 2017;50(2).
44. Hoeper MM, Kramer T, Pan Z, Eichstaedt CA, Spiesshoefer J, Benjamin N, et al. Mortality in pulmonary arterial hypertension: prediction by the 2015 European pulmonary hypertension guidelines risk stratification model. European Respiratory Journal. 2017;50(2):1700740.
45. Benza RL, Kanwar MK, Raina A, Scott JV, Zhao CL, Selej M, et al. Development and Validation of an Abridged Version of the REVEAL 2.0 Risk Score Calculator, REVEAL Lite 2, for Use in Patients With Pulmonary Arterial Hypertension. CHEST. 2021;159(1):337-46.
46. Hjalmarsson C, Kjellström B, Jansson K, Nisell M, Kylhammar D, Kavianipour M, et al. Early risk prediction in idiopathic <em>versus</em> connective tissue disease-associated pulmonary arterial hypertension: call for a refined assessment. ERJ Open Research. 2021;7(3):00854-2020.
47. Bouzina H, Rådegran G, Butler O, Hesselstrand R, Hjalmarsson C, Holl K, et al. Longitudinal changes in risk status in pulmonary arterial hypertension. ESC Heart Fail. 2021;8(1):680-90.
48. Kylhammar D, Hjalmarsson C, Hesselstrand R, Jansson K, Kavianipour M, Kjellström B, et al. Predicting mortality during long-term follow-up in pulmonary arterial hypertension. ERJ Open Research. 2021;7(2):00837-2020.
49. Boucly A, Weatherald J, Savale L, de Groote P, Cottin V, Prévot G, et al. External validation of a refined four-stratum risk assessment score from the French pulmonary hypertension registry. European Respiratory Journal. 2022;59(6):2102419.
50. Mayeux JD, Pan IZ, Dechand J, Jacobs JA, Jones TL, McKellar SH, et al. Management of Pulmonary Arterial Hypertension. Curr Cardiovasc Risk Rep. 2021;15(1):2.
51. Kadoglou NPE, Khattab E, Velidakis N, Gkougkoudi E, Myrianthefs MM. The Role of Echocardiography in the Diagnosis and Prognosis of Pulmonary Hypertension. Journal of Personalized Medicine. 2024;14(5):474.
52. Baggen VJM, Driessen MMP, Post MC, van Dijk AP, Roos-Hesselink JW, van den Bosch AE, et al. Echocardiographic findings associated with mortality ortransplant in patients with pulmonary arterial hypertension:A systematic review and meta-analysis. Neth Heart J. 2016;24(6):374-89.
53. Hulshof HG, Eijsvogels TMH, Kleinnibbelink G, van Dijk AP, George KP, Oxborough DL, et al. Prognostic value of right ventricular longitudinal strain in patients with pulmonary hypertension: a systematic review and meta-analysis. Eur Heart J Cardiovasc Imaging. 2019;20(4):475-84.
54. Liu K, Zhang C, Chen B, Li M, Zhang P. Association between right atrial area measured by echocardiography and prognosis among pulmonary arterial hypertension: a systematic review and meta-analysis. BMJ Open. 2020;10(9):e031316.
55. Shukla M, Park JH, Thomas JD, Delgado V, Bax JJ, Kane GC, et al. Prognostic Value of Right Ventricular Strain Using Speckle-Tracking Echocardiography in Pulmonary Hypertension: A Systematic Review and Meta-analysis. Can J Cardiol. 2018;34(8):1069-78.
56. de Liyis BG, Suastika LOS, Sutedja JC, Jagannatha GNP, Kosasih AM, Alamsyah AH. Prognostic values of right ventricular echocardiography functional parameters for mortality prediction in precapillary pulmonary hypertension: a systematic review and meta-analysis. Egypt Heart J. 2024;76(1):105.
57. Tello K, Axmann J, Ghofrani HA, Naeije R, Narcin N, Rieth A, et al. Relevance of the TAPSE/PASP ratio in pulmonary arterial hypertension. Int J Cardiol. 2018;266:229-35.
58. Tello K, Wan J, Dalmer A, Vanderpool R, Ghofrani HA, Naeije R, et al. Validation of the Tricuspid Annular Plane Systolic Excursion/Systolic Pulmonary Artery Pressure Ratio for the Assessment of Right Ventricular-Arterial Coupling in Severe Pulmonary Hypertension. Circ Cardiovasc Imaging. 2019;12(9):e009047.
59. Galiè N, Corris PA, Frost A, Girgis RE, Granton J, Jing ZC, et al. Updated treatment algorithm of pulmonary arterial hypertension. J Am Coll Cardiol. 2013;62(25 Suppl):D60-72.
60. Jaeschke R, Singer J, Guyatt GH. Measurement of health status. Ascertaining the minimal clinically important difference. Control Clin Trials. 1989;10(4):407-15.
61. Du H, Newton PJ, Salamonson Y, Carrieri-Kohlman VL, Davidson PM. A review of the six-minute walk test: its implication as a self-administered assessment tool. Eur J Cardiovasc Nurs. 2009;8(1):2-8.
62. Gabler NB, French B, Strom BL, Palevsky HI, Taichman DB, Kawut SM, et al. Validation of 6-minute walk distance as a surrogate end point in pulmonary arterial hypertension trials. Circulation. 2012;126(3):349-56.
63. Zelniker TA, Huscher D, Vonk-Noordegraaf A, Ewert R, Lange TJ, Klose H, et al. The 6MWT as a prognostic tool in pulmonary arterial hypertension: results from the COMPERA registry. Clin Res Cardiol. 2018;107(6):460-70.
64. Heresi GA, Rao Y. Follow-Up Functional Class and 6-Minute Walk Distance Identify Long-Term Survival in Pulmonary Arterial Hypertension. Lung. 2020;198(6):933-8.
65. Radchenko GD, Zhyvylo IO, Sirenko YM. Analysis of pulmonary hypertension patient survival after treatment in referral center (data of first Ukrainian register). Pulm Circ. 2019;9(2):2045894019845604.
66. Xiong W, Zhao Y, Xu M, Pudasaini B, Guo X, Liu J. A modified risk score in one-year survival rate assessment of group 1 pulmonary arterial hypertension. BMC Pulmonary Medicine. 2018;18(1):161.
67. Gall H, Felix JF, Schneck FK, Milger K, Sommer N, Voswinckel R, et al. The Giessen Pulmonary Hypertension Registry: Survival in pulmonary hypertension subgroups. J Heart Lung Transplant. 2017;36(9):957-67.
68. Zhao J, Wang Q, Liu Y, Tian Z, Guo X, Wang H, et al. Clinical characteristics and survival of pulmonary arterial hypertension associated with three major connective tissue diseases: A cohort study in China. Int J Cardiol. 2017;236:432-7.
69. Farber HW, Miller DP, McGoon MD, Frost AE, Benton WW, Benza RL. Predicting outcomes in pulmonary arterial hypertension based on the 6-minute walk distance. The Journal of Heart and Lung Transplantation. 2015;34(3):362-8.
70. Roy AK, McCullagh BN, Segurado R, McGorrian C, Keane E, Keaney J, et al. Detection of high-sensitivity troponin in outpatients with stable pulmonary hypertension identifies a subgroup at higher risk of adverse outcomes. J Card Fail. 2014;20(1):31-7.
71. Lee WT, Ling Y, Sheares KK, Pepke-Zaba J, Peacock AJ, Johnson MK. Predicting survival in pulmonary arterial hypertension in the UK. Eur Respir J. 2012;40(3):604-11.
72. Benza RL, Miller DP, Gomberg-Maitland M, Frantz RP, Foreman AJ, Coffey CS, et al. Predicting survival in pulmonary arterial hypertension: insights from the Registry to Evaluate Early and Long-Term Pulmonary Arterial Hypertension Disease Management (REVEAL). Circulation. 2010;122(2):164-72.
73. McLaughlin VV, Sitbon O, Badesch DB, Barst RJ, Black C, Galiè N, et al. Survival with first-line bosentan in patients with primary pulmonary hypertension. Eur Respir J. 2005;25(2):244-9.
74. McLaughlin VV, Gaine SP, Howard LS, Leuchte HH, Mathier MA, Mehta S, et al. Treatment goals of pulmonary hypertension. J Am Coll Cardiol. 2013;62(25 Suppl):D73-81.
Si tienes comentarios sobre el contenido de las guías de práctica clínica, puedes comunicarte con IETSI-EsSalud enviando un correo: gpcdireccion.ietsi@essalud.gob.pe

SUGERENCIAS
Si has encontrado un error en esta página web o tienes alguna sugerencia para su mejora, puedes comunicarte con EviSalud enviando un correo a evisalud@gmail.com